Bite Problems in Children and Their Footprint: How Are They Related?

Is it possible that the bite problems in children originate from their poor footprint? Although it may sound hard to believe, the postures of both structures are closely related.
Currently, dental malocclusions are the second most frequent disorder of the oral cavity in children, after cavities. For this reason, there’s great interest in discovering those factors that predispose children to their appearance in order to contribute to prevention.
Today, we’re going to tell you why children’s footprint problems have an impact on their bite and what you can do about it. Don’t miss it!
The relationship between bite problems in children and their footprint
Some studies that have analyzed the way people walk have found a direct relationship between podiatric alterations and spinal deviations, posture problems, neck disorders, and dental malocclusions. Therefore, abnormal stepping could be a predisposing factor for bite problems in children.
Depending on how we place our feet when stepping, we adapt the posture of the rest of the body to maintain balance. These unconscious compensations are what lead to other more distant structures developing a problem.
During childhood, the way in which we support our feet when stepping is strengthened. If these postures are incorrect and aren’t corrected during the growth period, they end up compromising the balance of the head and the location of the jaw. And with this, the development of the jaws and dental arches is altered, leading to malocclusion.
In a study conducted in 2018, a close relationship was determined between the pronated position of the foot (i.e., with the ankle bent toward the center of the body) and the appearance of the protrusion (advancement) of the lower jaw. This occlusal condition is classified as class III.
On the other hand, patients with flat feet and valgus feet (i.e., with the tip of the first toes tending toward the center of the body) may develop class II syndromes. In these cases, the bite is characterized by a protrusion of the upper jaw.
Also, bite disorders can lead to postural asymmetries in the rest of the body. When biting poorly, the muscles of the head, neck, shoulders, lower back, and legs are also affected. Ultimately, changes in gait are the result.

Types of gait and bite problems in children
Bite problems in children and gait problems are issues that health care professionals evaluate during routine visits. It’s common for physicians to observe the characteristics of the child’s feet and gait during the pediatric visit. At the same time, orthodontists corroborate the type of bite and detect any type of inconvenience having to do with it in the little ones.
At the same time, there’s a simple (and even fun) activity to implement at home in order to know the type of footprint that your little one has. While it has no diagnostic value, it may suggest that you need to talk to your pediatrician about it.
Paint the soles of your child’s feet with washable paint and have them step barefoot on a sheet of paper. By observing their footprints, you’ll be able to understand their feet better. We’ll tell you all the alternatives you may detect.
1. Normal footprint
This is the most common and is referred to as a normal pronator or neutral foot. The footprint is observed with the forefoot, the heel, and the outer half of the sole marked. The arch area is not imprinted on the paper.
The footprint is straight, with no inward or outward tendencies.
2. Flat footprint
By observing the footprint on the paper, you can notice if all or most of the sole is marked. This is due to the fact that the arch isn’t developed, and in these cases, we’re talking about flat feett.
Although this condition is to be expected in young children, it should correct itself with the passage of time. This type of footprint is related to sunken palates and class II malocclusions. Furthermore, flat feet have repercussions on the development of the entire locomotor system and require early intervention to avoid complications.
3. Cava footprint
In some footprints, you can observe that only the front part of the foot and the heel are marked. This type of footprint implies a very exaggerated curvature of the plantar arch and this is known as pes cavus.
It’s common that when walking, there’s a tendency to support the external (or lateral) part of the foot, which can be easily verified with the wear of the shoe on the outer sides.
As we’ve already mentioned, this type of footprint can be related to an advanced upper jaw and even to an ogival palate. Children who walk this way usually have an exaggerated lumbar curvature and when viewed from the side, it gives the impression that the neck and head are more inclined forward.
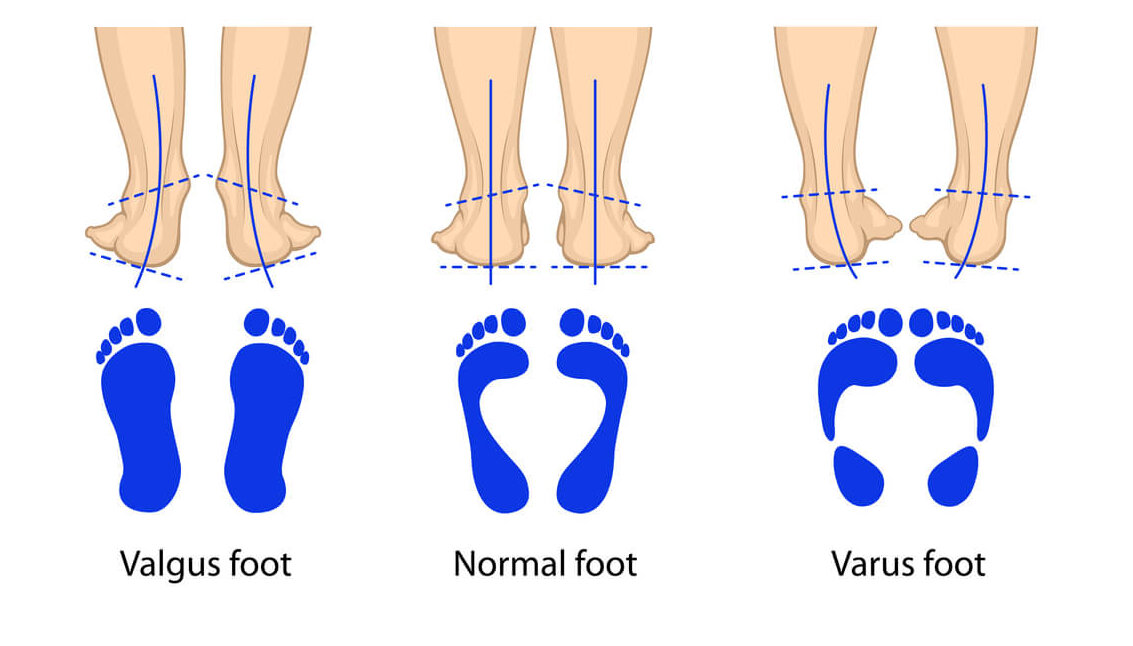
4. Valgus foot and rod
When the arch isn’t respected and the foot is bent extremely inward or outward, it’s assumed to be a malformation in the development of the extremities.
- The varus foot is characterized by being rotated inward. The arch and the heel are oriented towards the middle of the body and when the child walks, it seems like they walk on their ankles. This disorder is related to mandibular protrusion.
- On the other hand, the valgus foot has a deviation of the heels outward and the toes inward. In this case, if the foot were to settle on paper, the inner area would be marked, as both the arch and the heel are rotated outward. This gait is associated with Class II bite problems.
In both cases, the diagnosis is usually made in the first months of the child’s life, as it is very marked. In some cases, it’s corrected with orthopedics, and in the most severe cases, it may be necessary to resort to surgery and physiotherapy.
Bite problems in children
Malocclusions in children are a common problem that affects the oral functions of young children. Chewing, eating, speaking, and even smiling and interacting with their peers can be complicated if the bite is altered.
Jaws that are too far forward, too far back, open, or crossbites, crowding, diastemas, and overbites are some of the most common occlusion problems in children. And their causes are varied.
Heredity and genetics, oral habits, and tooth loss are some of the possible origins. And as we’ll tell you here, posture and gait also influence the genesis of bite problems in children.
Even so, not all malocclusions imply posture problems, just as not all abnormal plantar footprints lead to an altered bite.
Knowing the relationship between gait and bite problems in children helps to consider this association. An early diagnosis is always key to avoiding more severe problems. For this reason, dental and pediatric check-ups are the key to ensuring the well-being of the child and detecting any alteration in time.
Is it possible that the bite problems in children originate from their poor footprint? Although it may sound hard to believe, the postures of both structures are closely related.
Currently, dental malocclusions are the second most frequent disorder of the oral cavity in children, after cavities. For this reason, there’s great interest in discovering those factors that predispose children to their appearance in order to contribute to prevention.
Today, we’re going to tell you why children’s footprint problems have an impact on their bite and what you can do about it. Don’t miss it!
The relationship between bite problems in children and their footprint
Some studies that have analyzed the way people walk have found a direct relationship between podiatric alterations and spinal deviations, posture problems, neck disorders, and dental malocclusions. Therefore, abnormal stepping could be a predisposing factor for bite problems in children.
Depending on how we place our feet when stepping, we adapt the posture of the rest of the body to maintain balance. These unconscious compensations are what lead to other more distant structures developing a problem.
During childhood, the way in which we support our feet when stepping is strengthened. If these postures are incorrect and aren’t corrected during the growth period, they end up compromising the balance of the head and the location of the jaw. And with this, the development of the jaws and dental arches is altered, leading to malocclusion.
In a study conducted in 2018, a close relationship was determined between the pronated position of the foot (i.e., with the ankle bent toward the center of the body) and the appearance of the protrusion (advancement) of the lower jaw. This occlusal condition is classified as class III.
On the other hand, patients with flat feet and valgus feet (i.e., with the tip of the first toes tending toward the center of the body) may develop class II syndromes. In these cases, the bite is characterized by a protrusion of the upper jaw.
Also, bite disorders can lead to postural asymmetries in the rest of the body. When biting poorly, the muscles of the head, neck, shoulders, lower back, and legs are also affected. Ultimately, changes in gait are the result.
Types of gait and bite problems in children
Bite problems in children and gait problems are issues that health care professionals evaluate during routine visits. It’s common for physicians to observe the characteristics of the child’s feet and gait during the pediatric visit. At the same time, orthodontists corroborate the type of bite and detect any type of inconvenience having to do with it in the little ones.
At the same time, there’s a simple (and even fun) activity to implement at home in order to know the type of footprint that your little one has. While it has no diagnostic value, it may suggest that you need to talk to your pediatrician about it.
Paint the soles of your child’s feet with washable paint and have them step barefoot on a sheet of paper. By observing their footprints, you’ll be able to understand their feet better. We’ll tell you all the alternatives you may detect.
1. Normal footprint
This is the most common and is referred to as a normal pronator or neutral foot. The footprint is observed with the forefoot, the heel, and the outer half of the sole marked. The arch area is not imprinted on the paper.
The footprint is straight, with no inward or outward tendencies.
2. Flat footprint
By observing the footprint on the paper, you can notice if all or most of the sole is marked. This is due to the fact that the arch isn’t developed, and in these cases, we’re talking about flat feett.
Although this condition is to be expected in young children, it should correct itself with the passage of time. This type of footprint is related to sunken palates and class II malocclusions. Furthermore, flat feet have repercussions on the development of the entire locomotor system and require early intervention to avoid complications.
3. Cava footprint
In some footprints, you can observe that only the front part of the foot and the heel are marked. This type of footprint implies a very exaggerated curvature of the plantar arch and this is known as pes cavus.
It’s common that when walking, there’s a tendency to support the external (or lateral) part of the foot, which can be easily verified with the wear of the shoe on the outer sides.
As we’ve already mentioned, this type of footprint can be related to an advanced upper jaw and even to an ogival palate. Children who walk this way usually have an exaggerated lumbar curvature and when viewed from the side, it gives the impression that the neck and head are more inclined forward.
4. Valgus foot and rod
When the arch isn’t respected and the foot is bent extremely inward or outward, it’s assumed to be a malformation in the development of the extremities.
- The varus foot is characterized by being rotated inward. The arch and the heel are oriented towards the middle of the body and when the child walks, it seems like they walk on their ankles. This disorder is related to mandibular protrusion.
- On the other hand, the valgus foot has a deviation of the heels outward and the toes inward. In this case, if the foot were to settle on paper, the inner area would be marked, as both the arch and the heel are rotated outward. This gait is associated with Class II bite problems.
In both cases, the diagnosis is usually made in the first months of the child’s life, as it is very marked. In some cases, it’s corrected with orthopedics, and in the most severe cases, it may be necessary to resort to surgery and physiotherapy.
Bite problems in children
Malocclusions in children are a common problem that affects the oral functions of young children. Chewing, eating, speaking, and even smiling and interacting with their peers can be complicated if the bite is altered.
Jaws that are too far forward, too far back, open, or crossbites, crowding, diastemas, and overbites are some of the most common occlusion problems in children. And their causes are varied.
Heredity and genetics, oral habits, and tooth loss are some of the possible origins. And as we’ll tell you here, posture and gait also influence the genesis of bite problems in children.
Even so, not all malocclusions imply posture problems, just as not all abnormal plantar footprints lead to an altered bite.
Knowing the relationship between gait and bite problems in children helps to consider this association. An early diagnosis is always key to avoiding more severe problems. For this reason, dental and pediatric check-ups are the key to ensuring the well-being of the child and detecting any alteration in time.
All cited sources were thoroughly reviewed by our team to ensure their quality, reliability, currency, and validity. The bibliography of this article was considered reliable and of academic or scientific accuracy.
- World Health Organization. (2013). Oral health surveys: basic methods. World Health Organization.
- Rodríguez, S. G., Rodríguez, M. L., & Ramos, L. P. (2017). Modificaciones de la oclusión dentaria y su relación con la postura corporal en Ortodoncia. Revisión bibliográfica. Revista Habanera de Ciencias Médicas, 16(3), 371-386.
- Marchena-Rodríguez, A., Moreno-Morales, N., Ramírez-Parga, E., Labajo-Manzanares, M. T., Luque-Suárez, A., & Gijon-Nogueron, G. (2018). Relationship between foot posture and dental malocclusions in children aged 6 to 9 years: A cross-sectional study. Medicine, 97(19).
- Gómez Munilla, A. (2015). Correlación de maloclusión, huella plantar y posturología en el paciente adulto.
- Yong, Y. J. (2018). Relación de las anomalías dentomaxilo-faciales sagitales con la postura corporal y el apoyo plantar. Revista Médica Electrónica, 40(3), 602-614.
- Bazán Ponce de León, J. E. (2018). Relación de la Maloclusión, Clase II de Angle y el pie plano en niños de las Aldeas Infantiles de Huarochirí, 2011.
- Cumbres Tena, M. (2019). Dispositivo para analizar los parámetros que influyen en la pisada para corregir la supinación o pronación de un paciente.
- Espangler, L. G., Vázquez, W. E. D., Quevedo, Y. R., Martínez, M. R. L., & Sánchez, T. V. C. (2016). Relación de la postura corporal con las maloclusiones en adolescentes de un área de salud. Medisan, 20(12), 6001-6008.
- Jiménez Jiménez, J. (2017). Asociación entre maloclusiones dentales con problemas de actitud postural-columna vertebral en niños y adolescentes de 8 a 13 años.
- Montero Parrilla, J. M., Semykina, O., & Morais Chipombela, L. D. C. (2014). Trastornos temporomandibulares y su interacción con la postura corporal. Revista cubana de estomatología, 51(1), 3-14.
- Gogola, A., Saulicz, E., Matyja, M., Linek, P., Myśliwiec, A., Tuczyńska, A., & Molicka, D. (2014). Assessment of connection between the bite plane and body posture in children and teenagers. Developmental Period Medicine, 18(4), 453-458.
- Manfredini, D., Castroflorio, T., Perinetti, G., & Guarda‐Nardini, L. (2012). Dental occlusion, body posture and temporomandibular disorders: where we are now and where we are heading for. Journal of oral rehabilitation, 39(6), 463-471.
This text is provided for informational purposes only and does not replace consultation with a professional. If in doubt, consult your specialist.







