Osteogenesis Imperfecta in Children

Osteogenesis Imperfecta (OI) in children is a rare disease that doctors can detect quickly in prenatal screening. Although its incidence is low, it’s essential to know what it is and how it’s detected.
What is osteogenesis imperfecta in children?
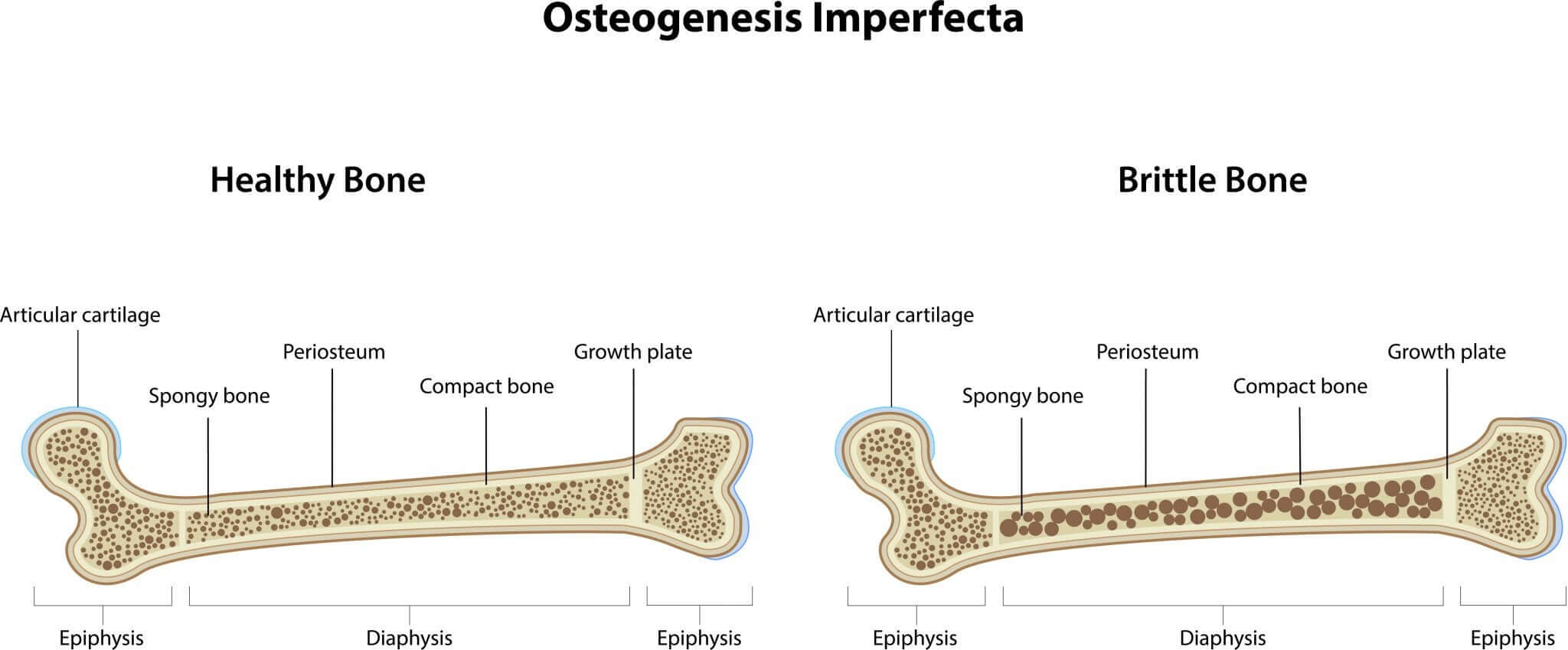
Osteogenesis imperfecta in children is an inherited connective tissue disease with a prevalence of 1 in 15,000 newborn babies. One of this disease’s main characteristics is a defective ossification of the skull and the high probability of a fracture occurring from trivial causes. This is mainly due to a lack of osteoblasts and osteoclasts, which lead to a lack of organic constituents.
There are several types of osteogenesis imperfecta, which are classified according to their level of severity. This can be I, II, III, IV, V or VI.
We should note here that there is a subdivision of types I and IV. These give rise to the groups I A and IV A, when there isn’t any opalescent dentine (a dental disorder, also called opalescent teeth), and I B and IV B, where there is.
Clinically, this pathology can appear in two ways: as congenital osteogenesis imperfecta and late osteogenesis imperfecta. The second is usually the most common form of the disease.
Types of OI in children
As mentioned above, osteogenesis imperfecta is divided into several types, from the mildest to the most severe condition. We’ll explain them in detail below:
OI type I
This type is considered the mildest of all. Symptoms include mild to moderate bone fragility, macrocephaly, triangular face, blue sclera, and fractures.
According to research conducted by the National Institute for the Protection of Exceptional Persons and the Institute for Research in Health Sciences, most cases show fractures at birth and, in fewer cases, during the first year of life.
OI type II
This type of osteogenesis imperfecta is considered the most serious. In fact, on many occasions, it can be fatal. This type is also divided into three groups, depending on the radiological characteristics.
The first is group II A, which is usually the most common and results in short bones, long bones, accordion tibia and rachitic rosary in the ribs. On the other hand, type II B also produces short, long, wide and wrinkled bones, but there’s no rachitic rosary in the ribs. Rib fractures may occur.
OI Type III
In the case of type III, we find that bone fragility can go from moderate to severe, and there’s often a deformity of limbs. Among the conditions that occur, we find macrocephaly, kyphoscoliosis and, on many occasions, dentinogenesis imperfecta and hearing loss.
OI type IV
This type of osteogenesis imperfecta produces intermediate bone fragility, between type I and type III. In general, the prognosis is positive; the sclera are normal and it’s autosomal dominant (AD).
OI Type V
In this type, it’s common to find fractures of long bones and vertebrae. As in the case of type IV, the sclera are normal and it’s AD.

OI type VI
In this case, fractures can occur between 4 and 18 months of age. The sclera are normal or light blue, no dentinogenesis imperfecta occurs, and vertebral fractures may occur.
What do studies say about osteogenesis imperfecta in children?
A study with the objective of analyzing the quality of life of patients with osteogenesis imperfecta was carried out by the National Hospital of Pediatrics. Dr. Juan P. Garrahan evaluated 65 families and 42 children, of which 35 had type I OI and 30 had type III-IV OI, between the ages of 2 and 18 years.
In the case of children between the ages of 2 and 4, they evaluated the parents’ vision. In addition, they helped the children between the ages of 5 and 7 to answer each of the evaluation questions.
As a result, in a total of 65 patients evaluated, the researchers determined that in children with type III-IV OI, there was a decrease in quality of life, mainly in physical matters. As for the results regarding parents, there was a lower perception of quality of life in the social domain.
Although osteogenesis imperfecta in children is rare, it’s essential to know what type of symptoms can occur and when we should see a specialist.
Osteogenesis Imperfecta (OI) in children is a rare disease that doctors can detect quickly in prenatal screening. Although its incidence is low, it’s essential to know what it is and how it’s detected.
What is osteogenesis imperfecta in children?
Osteogenesis imperfecta in children is an inherited connective tissue disease with a prevalence of 1 in 15,000 newborn babies. One of this disease’s main characteristics is a defective ossification of the skull and the high probability of a fracture occurring from trivial causes. This is mainly due to a lack of osteoblasts and osteoclasts, which lead to a lack of organic constituents.
There are several types of osteogenesis imperfecta, which are classified according to their level of severity. This can be I, II, III, IV, V or VI.
We should note here that there is a subdivision of types I and IV. These give rise to the groups I A and IV A, when there isn’t any opalescent dentine (a dental disorder, also called opalescent teeth), and I B and IV B, where there is.
Clinically, this pathology can appear in two ways: as congenital osteogenesis imperfecta and late osteogenesis imperfecta. The second is usually the most common form of the disease.
Types of OI in children
As mentioned above, osteogenesis imperfecta is divided into several types, from the mildest to the most severe condition. We’ll explain them in detail below:
OI type I
This type is considered the mildest of all. Symptoms include mild to moderate bone fragility, macrocephaly, triangular face, blue sclera, and fractures.
According to research conducted by the National Institute for the Protection of Exceptional Persons and the Institute for Research in Health Sciences, most cases show fractures at birth and, in fewer cases, during the first year of life.
OI type II
This type of osteogenesis imperfecta is considered the most serious. In fact, on many occasions, it can be fatal. This type is also divided into three groups, depending on the radiological characteristics.
The first is group II A, which is usually the most common and results in short bones, long bones, accordion tibia and rachitic rosary in the ribs. On the other hand, type II B also produces short, long, wide and wrinkled bones, but there’s no rachitic rosary in the ribs. Rib fractures may occur.
OI Type III
In the case of type III, we find that bone fragility can go from moderate to severe, and there’s often a deformity of limbs. Among the conditions that occur, we find macrocephaly, kyphoscoliosis and, on many occasions, dentinogenesis imperfecta and hearing loss.
OI type IV
This type of osteogenesis imperfecta produces intermediate bone fragility, between type I and type III. In general, the prognosis is positive; the sclera are normal and it’s autosomal dominant (AD).
OI Type V
In this type, it’s common to find fractures of long bones and vertebrae. As in the case of type IV, the sclera are normal and it’s AD.
OI type VI
In this case, fractures can occur between 4 and 18 months of age. The sclera are normal or light blue, no dentinogenesis imperfecta occurs, and vertebral fractures may occur.
What do studies say about osteogenesis imperfecta in children?
A study with the objective of analyzing the quality of life of patients with osteogenesis imperfecta was carried out by the National Hospital of Pediatrics. Dr. Juan P. Garrahan evaluated 65 families and 42 children, of which 35 had type I OI and 30 had type III-IV OI, between the ages of 2 and 18 years.
In the case of children between the ages of 2 and 4, they evaluated the parents’ vision. In addition, they helped the children between the ages of 5 and 7 to answer each of the evaluation questions.
As a result, in a total of 65 patients evaluated, the researchers determined that in children with type III-IV OI, there was a decrease in quality of life, mainly in physical matters. As for the results regarding parents, there was a lower perception of quality of life in the social domain.
Although osteogenesis imperfecta in children is rare, it’s essential to know what type of symptoms can occur and when we should see a specialist.
All cited sources were thoroughly reviewed by our team to ensure their quality, reliability, currency, and validity. The bibliography of this article was considered reliable and of academic or scientific accuracy.
- Herreros, M. B., Franco, R., & Ascurra, M. (2008). Osteogenesis imperfecta. Pediatría (Asunción), 35(1), 33-37.
- Fano, V., del Pino, M., Rodríguez Celin, M., Buceta, S., & Obregón, M. G. (2013). Osteogénesis imperfecta: estudio de la calidad de vida en los niños. Archivos argentinos de pediatría, 111(4), 328-331.
- Carbajal, P. M. (1964). Osteogénesis imperfecta. In Anales de la Facultad de Medicina (Vol. 47, No. 3, pp. 327-353). Universidad Nacional Mayor de San Marcos.
This text is provided for informational purposes only and does not replace consultation with a professional. If in doubt, consult your specialist.







